






















































Notification

THANK YOU FOR MAKING AN APPOINTMENT AT AIH.
Would you like to pre-register?
Please fill in the information below
Urgent
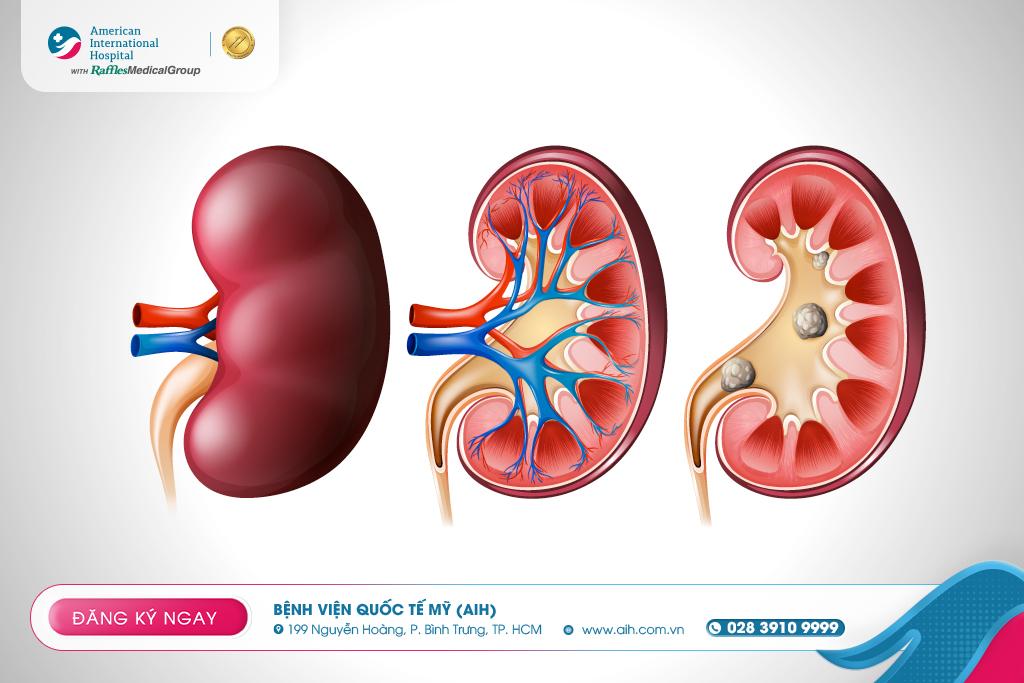
RENAL COLIC: DO NOT UNDERESTIMATE WARNING SIGNS OF NEPHROLITHIASIS

Kidney stones (nephrolithiasis) are solid masses formed from mineral crystals in urine, typically originating on the renal papillae and ranging in size from as small as a grain of sand to larger. When a stone detaches from its formation site and falls into the collecting system–ureter, it can cause partial or total obstruction. This leads to severe renal colic, which may be accompanied by hematuria, nausea/vomiting, urinary urgency, frequent urination, or urinary tract infection.
Classification
Classification by mineral composition:
Calcium stones (most common): primarily calcium oxalate; associated with hypercalciuria, hyperoxaluria; calcium phosphate is less common and may be associated with renal tubular acidosis.
Struvite stones (magnesium – ammonium – phosphate ± calcium carbonate), form due to urease-producing bacterial infections that lead to urine alkalinization.
Uric acid stones are favored by acidic urine (pH < 5,5) and hyperuricosuria, often seen in individuals with high protein diets or gout.
Cystine stones are rare and result from a genetic disorder called cystinuria.
Causes – Risk Factors
The general mechanism is urine supersaturated with crystals and/or a lack of crystallization inhibitors. Related factors include:
Dehydration leads to concentrated urine.
Diet: high oxalate (e.g., dark leafy greens, nuts) promotes calcium oxalate stones; high protein intake acidifies urine, promoting uric acid stones.
Underlying medical conditions: gout, hyperparathyroidism, urinary tract infections (struvite stones), inflammatory bowel disease or history of bowel surgery (increased urinary oxalate), renal tubular acidosis (calcium phosphate stones).
Family history/obesity: increases risk.
Symptoms
Renal colic suddenly occurs in the flank, radiating to the hypogastrium or inguine; macroscopic/microscopic hematuria, painful urination, burning urination, nausea/vomiting. If symptoms are accompanied by fever and chills, it may indicate an obstructive infection. Some stones may be asymptomatic and are only discovered incidentally during routine health check-ups.
Diagnosis
History taking – clinical examination, urine testing (erythrocytes, leukocytes/bacteria) and bloodwork (kidney function, complete blood count).
Imaging studies are for confirming the diagnosis and evaluating the location and size of the stones:
KUB X-ray may reveal radiopaque stones.
CT scans (or IVP in certain contexts, provide more detailed information when needed.
Stone analysis (if the stone is retrieved) and metabolic evaluation (usually involves blood tests and two 24-hour urine collections) are performed to plan long-term prevention.

Treatment
Some cases requiring early intervention: uncontrolled pain, severe vomiting, fever/infection, solitary kidney, impaired kidney function, or complete obstruction. The choice of treatment method depends on the size, location of the stone, severity of symptoms, presence of infection, and kidney function:
Watchful waiting – waiting for the stone to pass spontaneously: suitable for small stones with few symptoms; stones >5 mm is less likely to pass on their own and intervention should be considered.
Extracorporeal Shock Wave Lithotripsy (ESWL/"lithotripsy"): a non-invasive procedure that uses shock waves, localized by X-ray/ultrasound, to break the stone into small fragments to be expelled through the urinary tract.
Ureteroscopy: A small ureteroscope is introduced through the urethra and bladder, up into the ureter/calyxes and renal pelvis to access and address stones, typically under anesthesia.
Percutaneous Nephrolithotomy (PCNL): A small tunnel is created in the flank region into the kidney to remove/pulverize large or complex stones when ESWL/ureteroscopy is not suitable.
Latest advancements – current orientation
Minimally invasive and non-invasive: The American International Hospital is equipped with flexible ureteroscopes, incisionless lithotripsy, and modern Mini-PCNL percutaneous nephrolithotomy instruments with a very small incision (only about 3 - 4 mm) for laser lithotripsy. This is a highly effective technique for treating kidney stones, which can replace open surgery, resulting in less pain, less bleeding, faster recovery, and maximum protection of kidney function. After surgery, patients stay in the hospital for 2 - 3 days.
Personalized prevention: conduct a full metabolic evaluation (stone analysis, blood, and 24-hour urine analysis) to identify intervention targets such as increasing fluid intake (to achieve >2 liters of urine/day), adjusting salt/protein/oxalate, supplementing citrate, or using thiazide diuretics for hypercalciuria.

At the Department of Nephro-urology - Andrology, AIH, patients will receive comprehensive and personalized care from experienced urologists. With the support of modern diagnostic equipments, doctors can accurately diagnose complex diseases during the first examination, leading to the highest possibility of successful treatment.
AIH currently applies various treatment methods, from medication to minimally invasive surgeries such as endourology, laparoscopic surgery, etc., with the goal of bringing comfort and the fastest recovery to patients.
For consultation and to schedule an appointment with specialists in Nephrology - Urology - Andrology, please contact Hotline (028) 3910 9999 or INBOX our Fanpage https://m.me/aih.com.vn.
References:
Johns Hopkins Medicine
Raffles Medical Group
Raffles Medical Group


Leave a comment